The inflammation is caused by viruses, bacteria, irritants or allergens. The most common kind of rhinitis is allergic rhinitis,[5] which is usually triggered by airborne allergens such as pollen and dander.[6] Allergic rhinitis may cause additional symptoms, such as sneezing and nasal itching, coughing, headache,[7]fatigue, malaise, and cognitive impairment.[8][9] The allergens may also affect the eyes, causing watery, reddened, or itchy eyes and puffiness around the eyes.[7] The inflammation results in the generation of large amounts of mucus, commonly producing a runny nose, as well as a stuffy nose and post-nasal drip. In the case of allergic rhinitis, the inflammation is caused by the degranulation of mast cells in the nose. When mast cells degranulate, they release histamine and other chemicals,[10] starting an inflammatory process that can cause symptoms outside the nose, such as fatigue and malaise.[11] In the case of infectious rhinitis, it may occasionally lead to pneumonia, either viral or bacterial. Sneezing also occurs in infectious rhinitis to expel bacteria and viruses from the respiratory tract.
Rhinitis is very common. Allergic rhinitis is more common in some countries than others; in the United States, about 10–30% of adults are affected annually.[12] Mixed rhinitis (MR) refers to patients with nonallergic rhinitis and allergic rhinitis. MR is a specific rhinitis subtype. It may represent between 50 and 70% of all AR patients. However, true prevalence of MR has not been confirmed yet.[13]
Nonallergic rhinitis refers to rhinitis that is not due to an allergy. The category was formerly referred to as vasomotor rhinitis, as the first cause discovered was vasodilation due to an overactive parasympathetic nerve response. As additional causes were identified, additional types of nonallergic rhinitis were recognized. Vasomotor rhinitis is now included among these under the more general classification of nonallergic rhinitis.[17] The diagnosis is made upon excluding allergic causes.[18] It is an umbrella term of rhinitis of multiple causes, such as occupational (chemical), smoking, gustatory, hormonal, senile (rhinitis of the elderly), atrophic, medication-induced (including rhinitis medicamentosa), local allergic rhinitis, non-allergic rhinitis with eosinophilia syndrome (NARES) and idiopathic (vasomotor or non-allergic, non-infectious perennial allergic rhinitis (NANIPER), or non-infectious non-allergic rhinitis (NINAR).[19]
In vasomotor rhinitis,[20][21] certain nonspecific stimuli, including changes in environment (temperature, humidity, barometric pressure, or weather), airborne irritants (odors, fumes), dietary factors (spicy food, alcohol), sexual arousal, exercise,[22] and emotional factors trigger rhinitis.[23] There is still much to be learned about this, but it is thought that these non-allergic triggers cause dilation of the blood vessels in the lining of the nose, which results in swelling and drainage.
Non-allergic rhinitis can co-exist with allergic rhinitis, and is referred to as "mixed rhinitis".[24] The pathology of vasomotor rhinitis appears to involve neurogenic inflammation[25] and is as yet not very well understood. The role of transient receptor potential ion channels on the non-neuronal nasal epithelial cells has also been suggested. Overexpression of these receptors have influence the nasal airway hyper-responsiveness to non-allergic irritant environmental stimuli (e.g., extremes of temperature, changes in osmotic or barometric pressure).[26] Vasomotor rhinitis appears to be significantly more common in women than men, leading some researchers to believe that hormone imbalance plays a role.[27][28] In general, age of onset occurs after 20 years of age, in contrast to allergic rhinitis which can be developed at any age. Individuals with vasomotor rhinitis typically experience symptoms year-round, though symptoms may be exacerbated in the spring and autumn when rapid weather changes are more common.[17] An estimated 17 million United States citizens have vasomotor rhinitis.[17]
Drinking alcohol may cause rhinitis as well as worsen asthma (see alcohol-induced respiratory reactions). In certain populations, particularly those of East Asian countries such as Japan, these reactions have a nonallergic basis.[29] In other populations, particularly those of European descent, a genetic variant in the gene that metabolizes ethanol to acetaldehyde, ADH1B, is associated with alcohol-induced rhinitis. It is suggested that this variant metabolizes ethanol to acetaldehyde too quickly for further processing by ALDH2 and thereby leads to the accumulation of acetaldehyde and rhinitis symptoms.[30] In these cases, alcohol-induced rhinitis may be of the mixed rhinitis type and, it seems likely, most cases of alcohol-induced rhinitis in non-Asian populations reflect true allergic response to the non-ethanol and/or contaminants in alcoholic beverages, particularly when these beverages are wines or beers.[29] Alcohol-exacerbated rhinitis is more frequent in individuals with a history of rhinitis exacerbated by aspirin.[31]
A systematic review on non-allergic rhinitis reports improvement of overall function after treatment with capsaicin (the active component of chili peppers). The quality of evidence is low, however.[35]
Allergic rhinitis or hay fever may follow when an allergen such as pollen, dust, or Balsam of Peru[36] is inhaled by an individual with a sensitized immune system, triggering antibody production. These antibodies mostly bind to mast cells, which contain histamine. When the mast cells are stimulated by an allergen, histamine (and other chemicals) are released. This causes itching, swelling, and mucus production.
Symptoms vary in severity between individuals. Very sensitive individuals can experience hives or other rashes. Particulate matter in polluted air and chemicals such as chlorine and detergents, which can normally be tolerated, can greatly aggravate the condition.[citation needed]
Even if a person has negative skin-prick, intradermal and blood tests for allergies, they may still have allergic rhinitis, from a local allergy in the nose. This is called local allergic rhinitis.[38] Many people who were previously diagnosed with nonallergic rhinitis may actually have local allergic rhinitis.[39]
A patch test may be used to determine if a particular substance is causing the rhinitis.
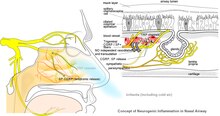
Pathological changes in non-allergic rhinitis[26]Mechanism of non-allergic rhinitis: Imbalance between sympathetic and parasympathetic components in the nasal mucous membrane[26]
Most prominent pathological changes observed are nasal airway epithelial metaplasia in which goblet cells replace ciliated columnar epithelial cells in the nasal mucous membrane.[26] This results in mucin hypersecretion by goblet cells and decreased mucociliary activity. Nasal secretion are not adequately cleared with clinical manifestation of nasal congestion, sinus pressure, post-nasal dripping, and headache. Over-expression of transient receptor potential (TRP) ion channels, such as TRPA1 and TRPV1, may be involved in the pathogenesis of non-allergic rhinitis.[41]
Association between rhinitis and asthma
Neurogenic inflammation produced by neuropeptides released from sensory nerve endings to the airways is a proposed common mechanism of association between both allergic and non-allergic rhinitis with asthma. This may explain higher association of rhinitis with asthma developing later in life.[42] Environmental irritants acts as modulators of airway inflammation in these contiguous airways. Development of occupational asthma is often preceded by occupational rhinitis. Among the causative agents are flours, enzymes used in processing food, latex, isocyanates, welding fumes, epoxy resins, and formaldehyde. Accordingly, prognosis of occupational asthma is contingent on early diagnosis and the adoption of protective measures for rhinitis.[43]
Diagnosis
The different forms of rhinitis are essentially diagnosed clinically.[clarification needed] Vasomotor rhinitis is differentiated from viral and bacterial infections by the lack of purulent exudate and crusting. It can be differentiated from allergic rhinitis because of the absence of an identifiable allergen.[44]
Evidence has been published from a few health apps for mobile devices that show potential to assist in the diagnosis of rhinitis and rhinosinusitis and to evaluate management and treatment adherence. While this shows promise for clinical management, as of 2022[update] few had been validated in the scientific literature, and even fewer included considerations for multimorbidity.[45][46]
Management
The management of rhinitis depends on the underlying cause.
Rhinitis comes from the Ancient Greekῥίςrhis, gen.: ῥινόςrhinos, "nose". Coryza comes through Latin from Ancient Greek κόρυζα. According to physician Andrew Wylie, "we use the term [coryza] for a cold in the head, but the two are really synonymous. The ancient Romans advised their patients to clean their nostrils and thereby sharpen their wits."[50]
^Bernstein, Jonathan A. (September 2010). "Allergic and mixed rhinitis: Epidemiology and natural history". Allergy and Asthma Proceedings. 31 (5): 365–369. doi:10.2500/aap.2010.31.3380. ISSN1539-6304. PMID20929601.
^ abcWheeler PW, Wheeler SF (September 2005). "Vasomotor rhinitis". American Family Physician. 72 (6): 1057–62. PMID16190503.
^Brown KR, Bernstein JA (June 2015). "Clinically relevant outcome measures of novel pharmacotherapy for nonallergic rhinitis". Current Opinion in Allergy and Clinical Immunology. 15 (3): 204–12. doi:10.1097/ACI.0000000000000166. PMID25899692. S2CID22343815.
^Silvers WS, Poole JA (February 2006). "Exercise-induced rhinitis: a common disorder that adversely affects allergic and nonallergic athletes". Annals of Allergy, Asthma & Immunology. 96 (2): 334–40. doi:10.1016/s1081-1206(10)61244-6. PMID16498856.
^Adelman D (2002). Manual of Allergy and Immunology: Diagnosis and Therapy. Lippincott Williams & Wilkins. p. 66. ISBN9780781730525.
^(Middleton's Allergy Principles and Practice, seventh edition.)
^Knipping S, Holzhausen HJ, Riederer A, Schrom T (August 2008). "[Ultrastructural changes in allergic rhinitis vs. idiopathic rhinitis]". Hno. 56 (8): 799–807. doi:10.1007/s00106-008-1764-4. PMID18651116. S2CID24135943.
^Rajan JP, Wineinger NE, Stevenson DD, White AA (March 2015). "Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: A meta-analysis of the literature". The Journal of Allergy and Clinical Immunology. 135 (3): 676–81.e1. doi:10.1016/j.jaci.2014.08.020. PMID25282015.
^Choi JH, Kim MA, Park HS (February 2014). "An update on the pathogenesis of the upper airways in aspirin-exacerbated respiratory disease". Current Opinion in Allergy and Clinical Immunology. 14 (1): 1–6. doi:10.1097/aci.0000000000000021. PMID24300420. S2CID205433452.
^Bernstein JA (October 2007). "Azelastine hydrochloride: a review of pharmacology, pharmacokinetics, clinical efficacy and tolerability". Current Medical Research and Opinion. 23 (10): 2441–52. doi:10.1185/030079907X226302. PMID17723160. S2CID25827650.
^Rondón C, Canto G, Blanca M (February 2010). "Local allergic rhinitis: a new entity, characterization and further studies". Current Opinion in Allergy and Clinical Immunology. 10 (1): 1–7. doi:10.1097/ACI.0b013e328334f5fb. PMID20010094. S2CID3472235.
^Rondón C, Fernandez J, Canto G, Blanca M (2010). "Local allergic rhinitis: concept, clinical manifestations, and diagnostic approach". Journal of Investigational Allergology & Clinical Immunology. 20 (5): 364–71, quiz 2 p following 371. PMID20945601.
^Ramey JT, Bailen E, Lockey RF (2006). "Rhinitis medicamentosa"(PDF). Journal of Investigational Allergology & Clinical Immunology. 16 (3): 148–55. PMID16784007.
^Scherer Hofmeier K, Bircher A, Tamm M, Miedinger D (April 2012). "[Occupational rhinitis and asthma]". Therapeutische Umschau. 69 (4): 261–7. doi:10.1024/0040-5930/a000283. PMID22477666.
^Wylie A (1927). "Rhinology and laryngology in literature and Folk-Lore". The Journal of Laryngology & Otology. 42 (2): 81–87. doi:10.1017/S0022215100029959. S2CID71281077.